Babies Walking Woth Hips Wie Baby Hip Dysplasia
Contents
- What is hip dysplasia
- Hip dysplasia complications
- Causes of hip dysplasia
- Risk factors for hip dysplasia
- Hip dysplasia symptoms
- Diagnosis of hip dysplasia
- Hip dysplasia treatment
- Living with hip dysplasia
- Hip dysplasia surgery
What is hip dysplasia
Hip dysplasia previously referred to as congenital (present at birth) dislocation of the hip can occur when a person's hip joint does not develop properly. Hip dysplasia is also called 'developmental dysplasia of the hip' or 'clicky hips'. Hip dysplasia is usually detected in babies, but adolescents and adults may also experience symptoms of undetected hip dysplasia later in life.
The hip joint consists of the top end of the thighbone (femur) which fits into a curved part of the pelvis (the acetabulum) like a ball and socket (see Figures 1 -3). The hip joint attaches the thigh bone (femur) to the pelvis. In developmental dysplasia of the hip the 'ball and socket' joint of the hips doesn't properly form in babies and young children – the acetabulum is too shallow so the femoral head isn't held tightly in place, the hip joint is loose becomes dislocated or unstable. In severe cases, the femur can come out of the socket (dislocate).
Hip dysplasia in babies is more common if the baby had a breech birth or if there is a family history of the condition. It is more common in girls and firstborn children.
Hip dysplasia diagnosed early in life can be corrected and usually fixed completely. But if not treated in childhood, hip dysplasia can damage the joint over the years and is a leading cause of hip pain and arthritis in older people. People with hip dysplasia may eventually need a hip replacement.
Developmental dysplasia of the hip may affect one or both hips but the left hip is affected three times more often than the right hip. Hip dysplasia is also more common in girls and firstborn children. Approximately one in every 600 girls is affected, compared to just one in 3,000 boys. About 1 or 2 in every 1,000 babies have developmental dysplasia of the hip that needs treating.
Developmental dysplasia of the hip is also more common in babies born with particular disorders, including cerebral palsy and spina bifida. There is a family history of developmental dysplasia of the hip in one third of cases.
The signs and symptoms include:
- reduced joint mobility
- a low clunking sound can be heard when the leg is gently rotated, which is the sound of the femur engaging the socket
- the stretch of skin between the anus and the genitals (perineum) is unusually wide.
For unilateral (one-sided) dislocation, symptoms include:
- The skin creases of the buttocks don't match.
- One knee joint looks higher than the other.
Routine checks for hip dysplasia
Babies are routinely checked at birth to make sure their hip joints are properly positioned. The baby is laid on its back, and the doctor rotates each leg at the hip to ensure full joint mobility. A dislocated hip doesn't have a full range of movement and tends to make a clicking or clunking sound as the ball of the femur moves in and out of the socket.
An ultrasound is usually performed to confirm the diagnosis and help determine the extent of the dislocation. X rays, CT scans and magnetic resonance imaging (MRI) scans may also be used.
Around 95 per cent of babies born with developmental dysplasia of the hip can be successfully treated.
Without treatment, developmental dysplasia of the hip may lead to problems later in life, including:
- developing a limp
- hip pain – especially during the teenage years
- painful and stiff joints (osteoarthritis)
With early diagnosis and treatment, most children are able to develop normally and have a full range of movement in their hip.
Hip dysplasia complications
Later in life, hip dysplasia can damage the soft cartilage (labrum) that rims the socket portion of the hip joint. This is called a hip labral tear. Hip dysplasia also can make the joint more likely to develop osteoarthritis. This occurs because of higher contact pressures over a smaller surface of the socket. Over time, this wears away the smooth cartilage on the bones that helps them glide against each other as the joint moves.
Figure 1. Hip joint
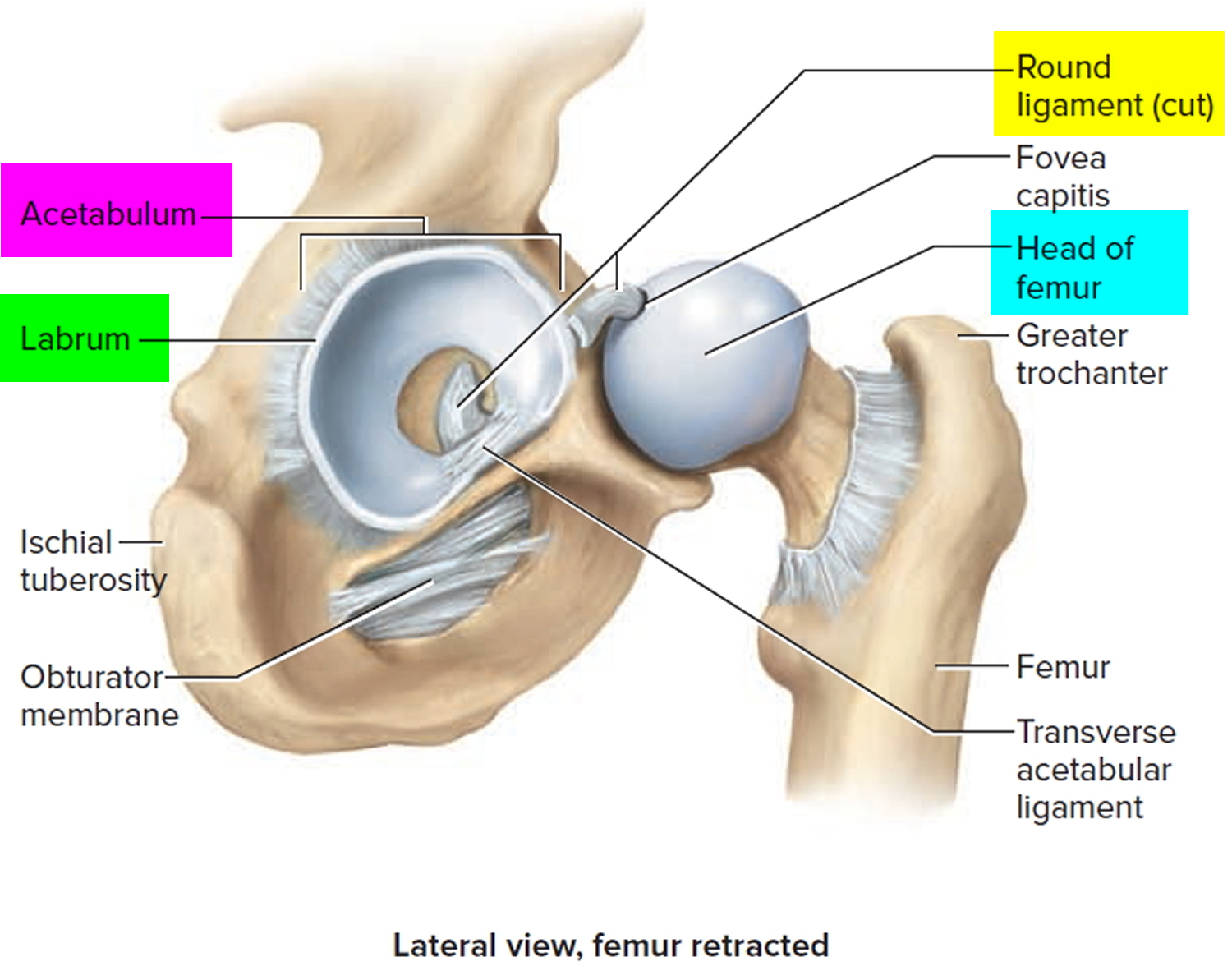
Figure 2. Hip joint frontal section
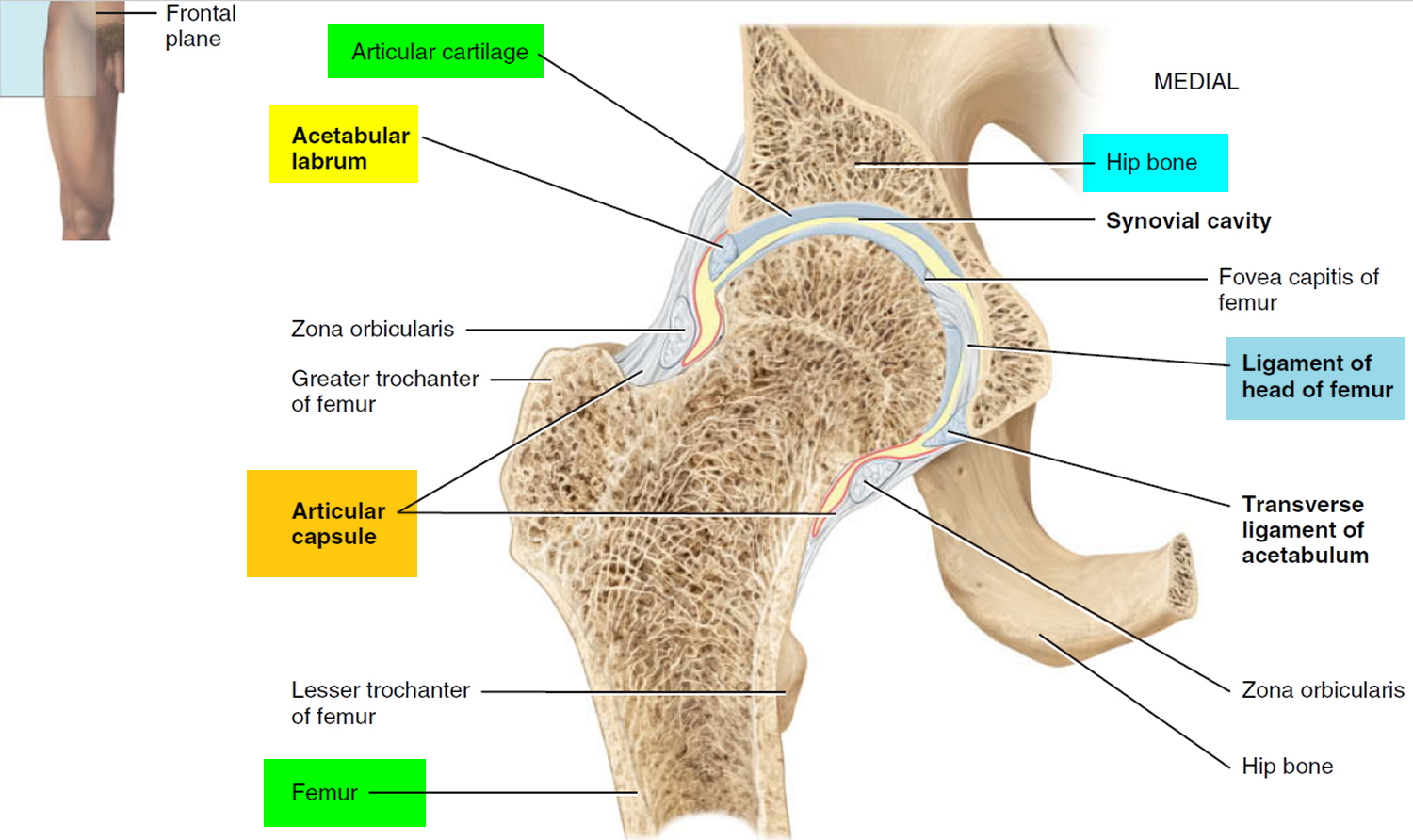
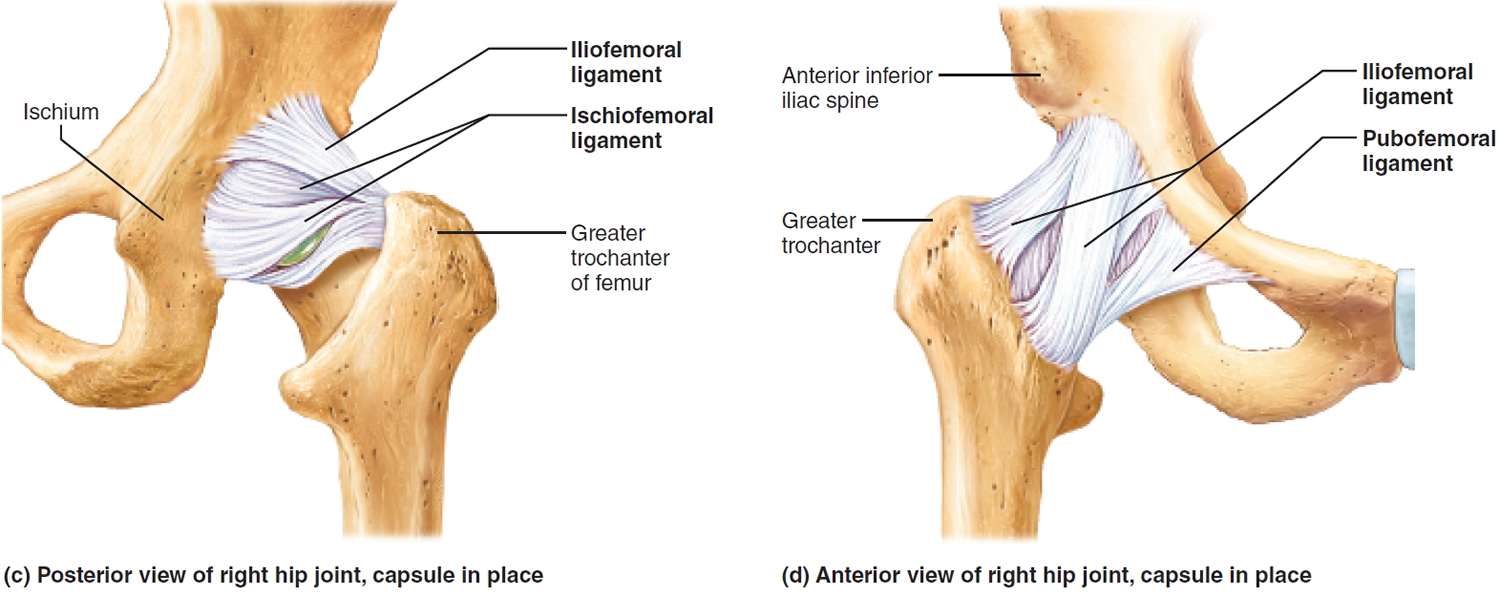
Figure 3. Hip joint ligaments
Causes of hip dysplasia
At birth, the hip joint is made of soft cartilage that gradually hardens into bone. The ball and socket need to fit together well because they act as molds for each other. If the ball isn't seated firmly into the socket, the socket will not fully form around the ball and will become too shallow.
During the final month before birth, the space within the womb can become so crowded that the ball of the hip joint moves out of its proper position, which results in a shallower socket.
There are many causes of hip dysplasia, factors that may reduce the amount of space in the womb include both genetic and environmental:
- Family history – around one third of babies with hip dysplasia have a blood relative who also had the condition
- Congenital disorders – hip dysplasia is more common in babies with disorders such as cerebral palsy and spina bifida
- Breech delivery – being born feet first can put considerable stress on the baby's hip joints
- Multiple babies – crowding inside the womb may dislocate the hip
- First-time mother – the inexperienced uterus and vagina may cause a difficult or prolonged delivery
Risk factors for hip dysplasia
Hip dysplasia tends to run in families and is more common in girls. The risk of hip dysplasia is also higher in babies born in the breech position or with foot deformities.
Hip dysplasia symptoms
Signs and symptoms vary by age group. In infants, you might notice that one leg is longer than the other. Once a child begins walking, a limp may develop. During diaper changes, one hip may be less flexible than the other.
Hip dysplasia in babies is not painful. Symptoms include:
- a hip joint that clicks when it's rotated
- uneven legs or skin creases near the buttocks
- late sitting or walking
- uneven walking
In teenagers and young adults, hip dysplasia can cause painful complications such as osteoarthritis or a hip labral tear. The main symptom of hip dysplasia cause activity-related groin pain. In some cases, you might experience a sensation of instability in the hip. It's common after sport and can be worse when you're standing up from a seated position, climbing in and out of a car, going downstairs, or if you suddenly rotate your hip.
Diagnosis of hip dysplasia
All newborn babies are examined for hip dysplasia in their first few days of life. These tests are repeated again at 6 weeks and at every appointment with the doctor or child and family health nurse. If they detect a problem or if your baby is at high risk of hip dysplasia, they may order an ultrasound.
In older children and adults, a physical examination and an ultrasound are used to diagnose the condition. An MRI or CT scan may be necessary to have a closer look at the acetabulum and assess any damage.
Hip dysplasia treatment
Treatment depends on your age, how severe the condition is, and whether you have developed arthritis.
A baby born with a developmental dysplasia of the hip can be successfully treated with a Pavlik harness for 6 to 10 weeks may help the hip develop normally. This device holds the joint in place while the baby's skeleton grows and matures. Subsequent x-rays will track the hip joint's progress. The Pavlik harness is effective in over 85 per cent of cases. Pavlik harness doesn't work as well for babies older than 6 months. Instead, the doctor may move the bones into the proper position and then hold them there for several months with a full-body cast. Sometimes surgery is needed to fit the joint together properly.
Most babies will require the Pavlik harness for between six and 12 weeks, and do not appear to be distressed by its use.
A small number of babies may need to have surgery or spend time in a plaster cast.
Most babies born with successfully treated hip dysplasia don't have any hip problems in later life. However, some may develop arthritis in the affected joint in their later years.
Figure 4. Pavlik harness
 Safe wrapping of baby
Safe wrapping of baby
In some babies, the ligaments around the hip joint are loose, which in most circumstances, corrects during the first few months of life. Research has shown that tight wrapping with the legs held straight can lead to hip dysplasia and dislocation.
When wrapping your baby, always remember to leave enough room in the wrap for the legs to move freely. Your baby's legs should be able to bend at the hips with their knees apart.
Older babies with developmental dysplasia of the hip
If a baby is diagnosed with a dislocated hip when they are six months old or more, then an anesthetic will be required before the hip is manipulated into its proper position. An operation may also be needed. A hip cast applied after surgery helps to keep the hip joint in place, and subsequent x-rays will track the hip joint's progress.
Later diagnosis of developmental dysplasia of the hip
Sometimes, a child isn't diagnosed with developmental dysplasia of the hip until they are two or three years of age. Symptoms may include a distinct waddling gait, one hip lower than the other, a limp, and walking on tiptoe.
Complications of untreated developmental dysplasia of the hip in an older child may include stability problems with the knee joints and injury to nerves supplying the femur (the thigh bone – between the hip and the knee).
Adolescents and adults with hip dysplasia
Milder cases of hip dysplasia might not start causing symptoms until a person is a teenager or young adult. Hip dysplasia can damage the cartilage lining the joint, and it can also hurt the soft cartilage (labrum) that rims the socket portion of the hip joint. This is called a hip labral tear.
In adolescents and adults, the aim of treatment is to preserve the hip for as long as possible. You may receive anti-inflammatory medicines, steroid injections and physiotherapy to help manage the condition.
Surgery can sometimes be used to reposition the acetabulum or repair the cartilage. But in some cases, the person may need a hip replacement.
Living with hip dysplasia
Gently moving and stretching the hip will help to keep it lubricated and moving well. A physiotherapist can give you an exercise plan. Physical activity and strengthening exercises will help you stay healthy, but avoid running and impact sports as they put too much pressure on the hip joint.
Walking with a cane may help in the later stages of hip dysplasia. One to 2 of every 5 adults with hip dysplasia develop osteoarthritis, a leading cause of disability.
Hip dysplasia surgery
Your doctor may recommend surgery if your child is experiencing pain and has limited damage to his or her articular cartilage. The surgical procedure most commonly used to treat hip dysplasia is an osteotomy. "Osteotomy" literally means "cutting of the bone." In an osteotomy, the doctor reshapes and reorients the acetabulum and/or femur so that the two joint surfaces are in a more normal anatomic position.
There are different types of osteotomies that can be performed to treat hip dysplasia. The specific procedure your doctor recommends will depend on a number of factors, including:
- Your child's age
- The severity of the dysplasia
- The extent of damage to the labrum
- Whether osteoarthritis is present
- The number of remaining growing years
Periacetabular osteotomy. Currently, the osteotomy procedure most commonly used to treat adolescent hip dysplasia is a periacetabular osteotomy. "Periacetabular" means "around the acetabulum."
In most cases, periacetabular osteotomy takes from 2-3 hours to perform. During the surgery, the doctor makes four cuts in the pelvic bone around the hip joint to loosen the acetabulum. He or she then rotates the acetabulum, repositioning it into a more normal anatomic position over the femoral head. The doctor will use x-rays to direct the bony cuts and to ensure that the acetabulum is repositioned correctly. Once the bone is repositioned, the doctor inserts several small screws to hold it in place until it heals.
Figure 5. Periacetabular osteotomy
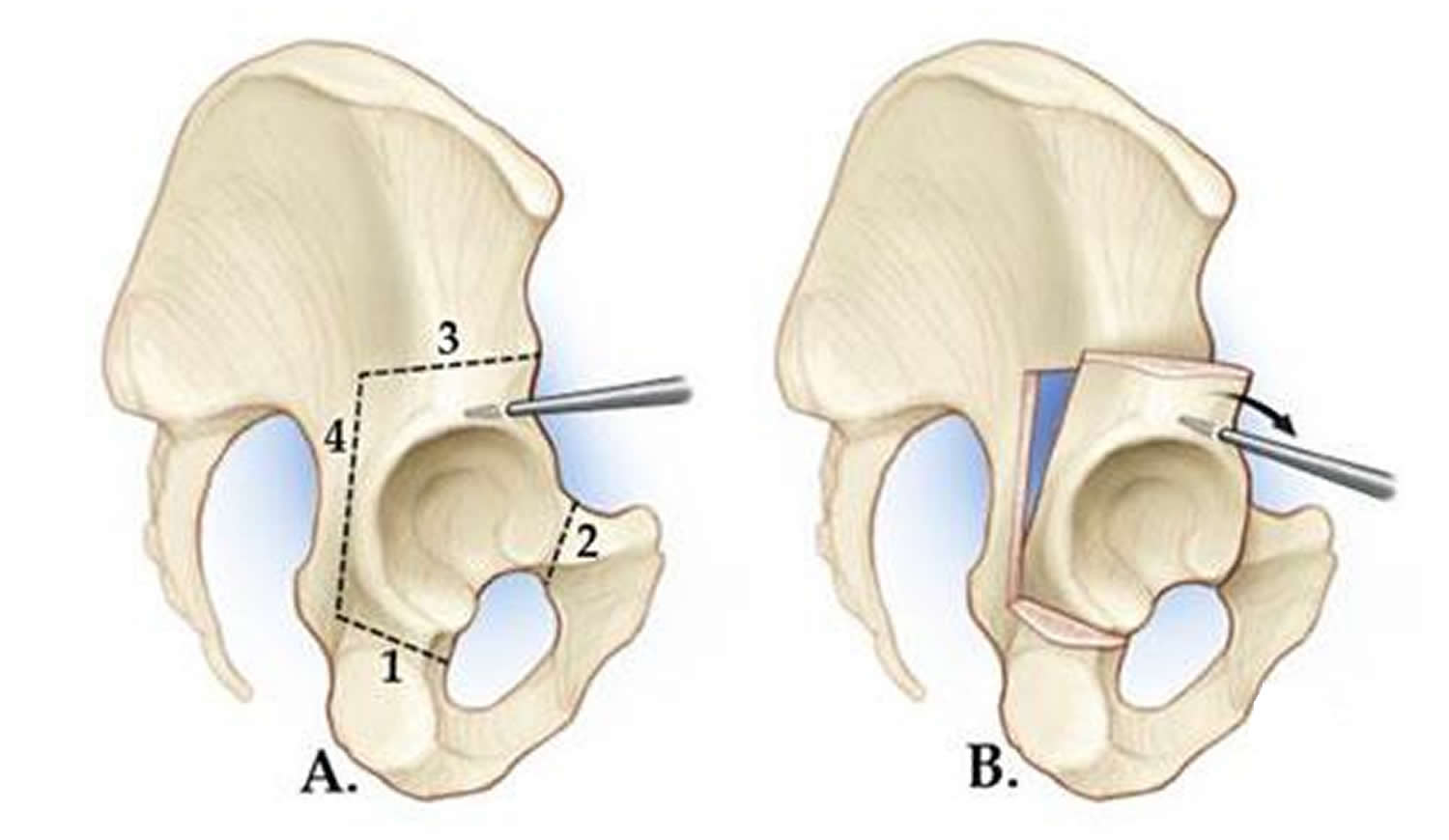 Note: (A) In a periacetabular osteotomy, four cuts are made in the pelvic bone. (B) The doctor uses a specialized tool to manipulate the bone fragment to gain access to the acetabulum.
Note: (A) In a periacetabular osteotomy, four cuts are made in the pelvic bone. (B) The doctor uses a specialized tool to manipulate the bone fragment to gain access to the acetabulum.
Figure 6. Periacetabular osteotomy
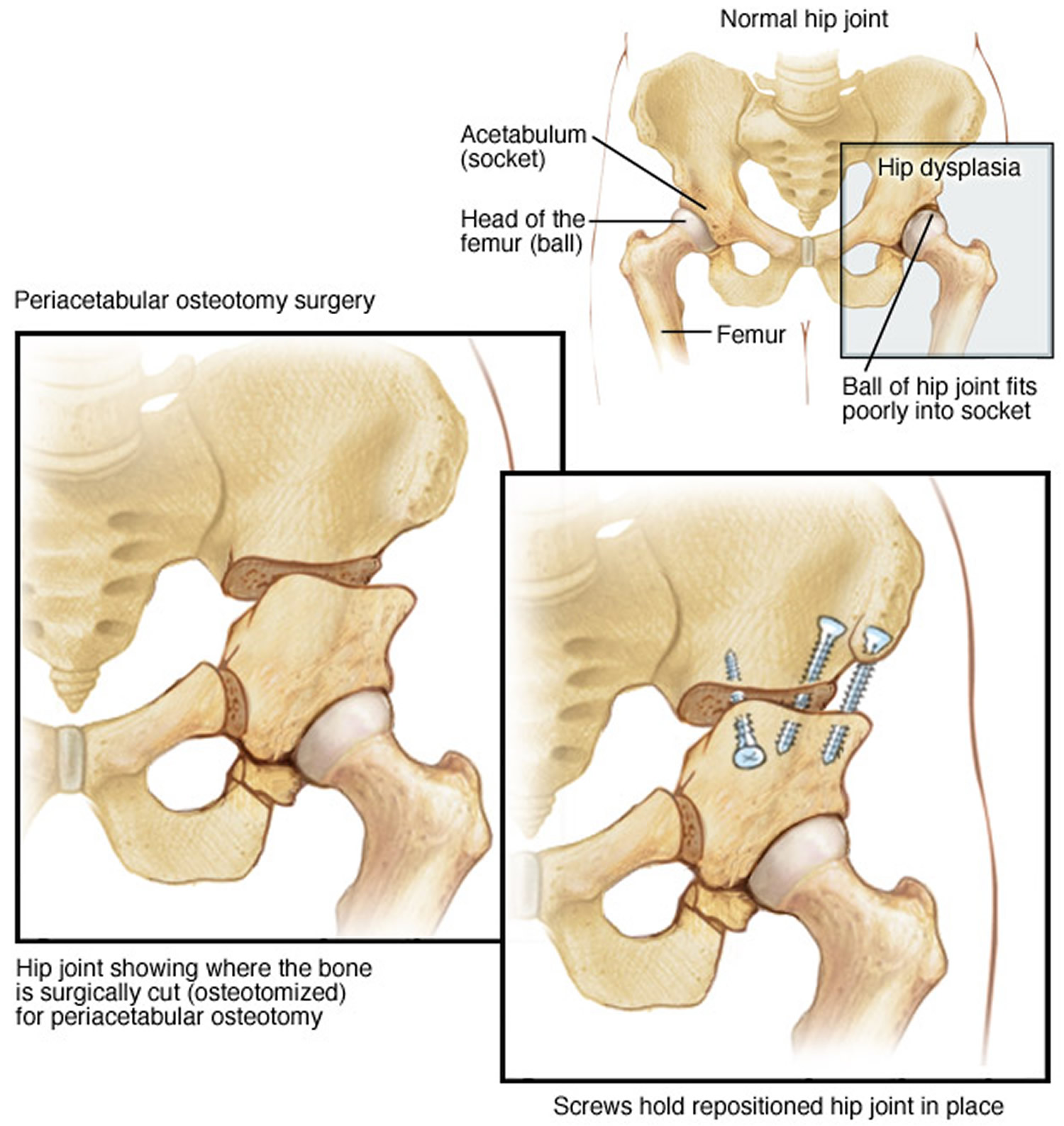
Figure 7. In this x-ray image, the acetabulum has been repositioned using a periacetabular osteotomy, and the bones are held in place with screws.

Arthroscopy. In conjunction with periacetabular osteotomy, your doctor may use hip arthroscopy to repair a torn labrum. During arthroscopy, the doctor inserts a small camera, called an arthroscope, into the joint. The camera displays pictures on a television screen, and your doctor uses these images to guide miniature surgical instruments. Arthroscopic procedures may include:
- Labral refixation. In this procedure, the doctor trims the torn and frayed tissue around the acetabular rim and reattaches the torn labrum to the bone of the rim.
- Debridement. In some cases, simply removing the torn or weakened labral tissue can provide pain relief.
Complications
As with any surgical procedure, there are risks involved with periacetabular osteotomy. Your doctor will discuss each of the risks with you and will take specific measures to help avoid potential complications.
Although the risks are low, the most common complications include:
- Infection
- Blood clots
- Injuries to blood vessels and nerves
- Persistent hip pain
- Failure of the osteotomy to heal
Recovery
Your child will remain in the hospital for 2 to 4 days after surgery. During this time, he or she will be monitored and given pain medication.
In most cases, full weight-bearing will not be allowed on the operated leg for 6 weeks to 3 months while the bones heal in their new position. During this time, your child will need to use crutches.
About 6 weeks after surgery, your child will have a follow-up visit with the doctor. X-rays will be taken so that the doctor can see how well the periacetabular osteotomy has healed. During your visit, the doctor will determine when it is safe to put weight on the leg and when physical therapy can begin. The physical therapist will show your child specific exercises to help maintain range of motion and restore strength and flexibility in the hip joint.
Outcomes
Periacetabular osteotomy is usually successful in delaying the need for an artificial hip joint and relieving pain. Whether or not a total hip replacement will be needed in the future depends on a number of factors, including the degree of osteoarthritis that was present in the joint when the periacetabular osteotomy was performed.
Babies Walking Woth Hips Wie Baby Hip Dysplasia
Source: https://healthjade.com/hip-dysplasia/
0 Response to "Babies Walking Woth Hips Wie Baby Hip Dysplasia"
Post a Comment